Common side effects of routine orthodontic mechanics
Common Side Effects of Routine Orthodontic Mechanics
The application of simple orthodontic mechanics often result in side effects that move teeth in directions that are difficult to predict. However, with an understanding of some basic wire-bracket relationships combined with the mechanical principles that underlie how teeth move, these seemingly bizarre movements can be not only predicted, but also eliminated. In this article, we will focus on two very common types of tooth movement that occur in the routine application of orthodontic forces. Although the interplay between these movements complicates understanding of the reasons behind these movements, the final result of the force systems can be understood and accounted for.
The first common movement occurs because orthodontic forces are rarely directed through the center of resistance of the teeth. Any force that is applied away from the center of resistance of a body produces a rotational tendency, or moment, on that body(1). Dr. Tom Mulligan, in his book “Common Sense Mechanics”, refers to this phenomenon as the “cue ball concept.” (2). If you wish to explore this concept in greater detail, you can refer to Mulligan’s textbook, which is listed as a reference at the end of this article. For our purposes, remember that any time an intrusive force is placed on a tooth, the moment produced creates a tendency for the crown of that tooth to flare. Conversely, when an extrusive force is applied to a tooth, the moment produced creates a tendency for the crown of that tooth to upright or roll lingually.
For example, when opening the bite with a reverse curve arch wire on the lower arch, the extrusive force on the molars, which is applied away from the center of resistance, results in a moment that rotates the crown of the tooth in a lingual direction. Additionally, the intrusive force placed on the incisors (again, the force is applied away from the center of resistance) results in a moment that can result in labial crown movement.
Expression of these side effects can lead to problems in the correction of malocclusions. For example, if, in an effort to open a deep bite, a practitioner places compensating curve in an upper arch wire, the rotational tendency as a result of the forces placed on the upper molars would produce a tendency for those molar crowns to roll to the lingual. This could result in a narrowing of the upper arch width. Since narrow upper arches are often associated with a retrusive mandibular position (3), this change in arch width could make a Class II problem worse. Additionally, the same wire, due to the intrusive force placed on the anterior teeth, could result in flaring of the anterior teeth. Clinically, spaces may appear between the anterior teeth after these forces are applied. So, a compensating curve applied to an upper arch in effort to open the bite could cause a serious worsening of a Class II malocclusion.
The second common movement occurs as a result of the angle of entry of a wire into a bracket. Dr. Gerry Samson identifies the potential problems as a result of angle of entry when he says “The greatest angle of entry determines the greatest moment of couple which determines the equilibrium forces.”(4)
This very important quote can be best understood by breaking it down into its component parts. First, let us explore the concept of angle of entry.

The angle of entry of the wire to the tooth can be affected by the malocclusion, archwire bends, and by the tip built into the pre-adjusted bracket. Most often, the greatest angle of wire entry occurs on the upper canine. Many malocclusions have mesially tipped upper canines, while many malocclusions have distally tipped upper canines. Additionally, because in the pre-adjusted appliance the canine bracket has the greatest tip built in, the net result is a wide variety of wire angles of entry which can profoundly change the movements that will be expressed as leveling and aligning occur.
The second portion of Dr. Samson's quote relates to the greatest moment of couple. Dr. Samson defines a couple as “equal and opposite forces (separated by a perpendicular distance) that are not in a straight line.” (5) The picture below demonstrates a common example of a couple.

In the bracket/wire relationship in the drawing, the “equal and opposite forces” are a result of the wire contacting the bracket slot in the upper left portion of the slot and the lower right portion of the slot. The two forces produced as a result of this contact are equal, and are directed in opposite directions (depicted by the arrows in the drawing on the right).The result of this force system is a rotation of the tooth in a mesial or distal direction (tipping of the tooth, if we use the orthodontic term).
.
The final part of Dr. Samson's quote refers to the equilibrium forces. This can be best understood by again viewing the picture above. Because of the angle of entry of the wire into the slot, the wire will be positioned above the brackets to the left of the slot in the picture, and below the brackets to the right of the slot in the picture. Deflecting that wire into those slots will result in (let us assume for discussion that this is an upper right canine bracket) an intrusive force to the teeth to the left of the slot (again, if this is an upper right canine those teeth would be the pre-molars and molars) and an extrusive force to the teeth to the right of the slot (anterior teeth in our example).
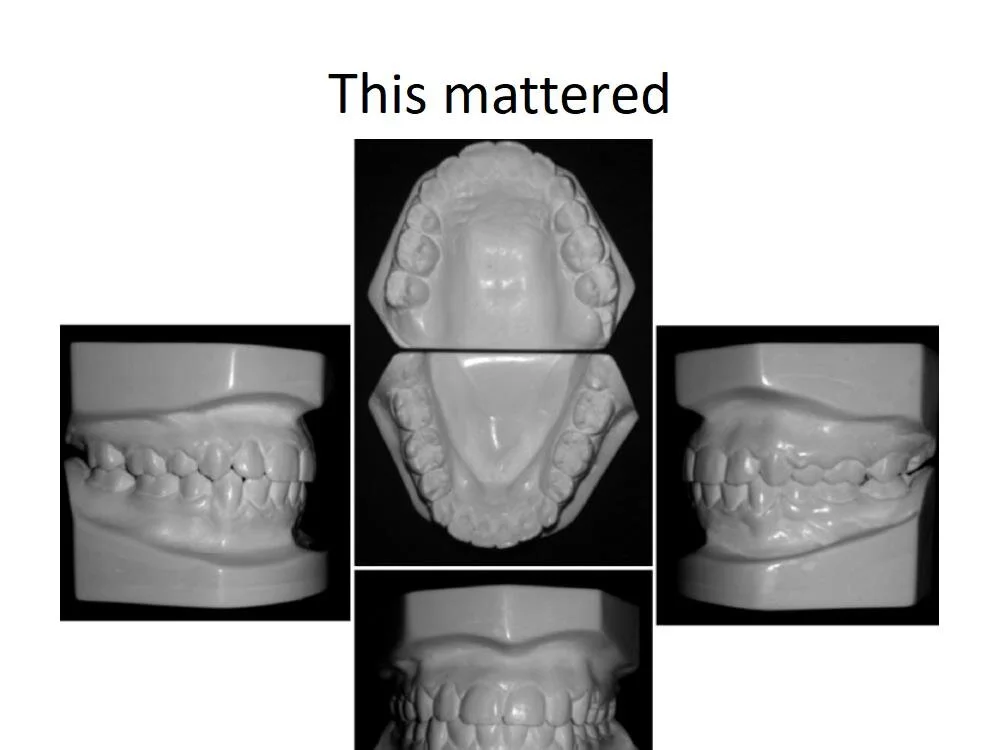
Now here is where the prediction of tooth response gets tricky. The intrusive and extrusive forces applied to the teeth as a result of the angle of entry will, because they are forces applied away from the center of resistance, result in rotational tendencies. To explain this, let us look at another example. The picture below is a pretreatment photo of a deep bite patient.

Let’s study this malocclusion. First, where will the greatest angle of wire entry be? Look at the canine and imagine a bracket placed on that tooth. Clearly, because of the mesially tipped canine combined with the large amount of tip in the pre-adjusted canine bracket, the angle of wire entry onto that tooth will be a lot larger than on any other tooth. Therefore, this angle of entry will determine equilibrium (where the teeth will go). Visualize a straight wire placed through the canine bracket. Where would that wire lie? Well, it would lie significantly gingivally to the anterior teeth and significantly occlusally to the posterior teeth. Next, ask yourself what forces will be imparted to those teeth as a result of the position of this wire? The answer is an intrusive force to the upper anterior teeth and an extrusive force to the upper posterior teeth. Finally, what kind of tooth movement will occur as a result of these forces? The answer is the moment as a result of the intrusive force on the anterior teeth will result in flaring of those crowns and the moment as a result of the extrusive force on the upper posterior teeth will result in molar and bicuspid lingual crown rotation. So the net result should be bite opening, flaring of the upper anterior teeth and lingual movement (rolling in) of the upper posterior crowns. Let’s look at what happened. Here is the initial bracketing photo and the picture after the first three months of treatment.

After one month of treatment

After 2 months of treatment

After 3 months of treatment
What happened in this initial leveling and aligning and is it predictable? The bite opened and the upper anterior teeth flared. This is exactly what should have happened. Additionally, the arch width narrowed in the posterior. Look at the bicuspid position pretreatment and after three months. Evaluate the amount of overjet in the bicuspid area. Clearly, these crowns rotated lingually.
This case demonstrates in cases with mesially inclined upper canine crowns, bite opening can occur quickly. Let’s look at another example.


Pretreatment


After one month (top) and 2 months (bottom)
What happened in this treatment? Clearly, the bite opening did not progress as easily as it did in the previous case. Why not? The answer can be discerned by examining the angle of wire entry onto the upper canine. In this case, the distally inclined canine resulted in the wire sitting below the brackets in the anterior teeth, which resulted in an extrusive force to those teeth. Bite deepening and lingual anterior crown rotation (due to the moment produced) occurred. Also, study the position of the upper right 2nd bicuspid. It is much more lingually inclined in the pretreatment photo than it is after one month of treatment. Why did this happen? An understanding of moments and forces provides the answer. The wire angle of entry on the canine bracket resulted in the wire sitting above the posterior brackets. When this wire was engaged, the result was in intrusive force to the posterior teeth. The resulting moment leads to the tendency for buccal crown rotation. The 2nd bicuspid rotated so far to the buccal that it almost went to reverse cross bite.
Understanding the “hows” and “whys” of the side effects of routine orthodontic mechanics allow the practitioner to take steps to emphasize the side effects that will help a particular malocclusion and minimize the side effects that may worsen the malocclusion. For example, in an open bite case with mesially inclined upper canines (see photo below), the leveling and aligning that will occur could worsen the open bite.

To mitigate these effects, the practitioner may want to position the anterior brackets more to the gingival than the original malocclusion would dictate. The anterior gingival bracket position compensates for the bite opening that is common with mesially inclined upper canines.
One common way to help control deleterious side effects is to change the inclination of the canine brackets to make the angle of entry less severe. Another solution is to simply level and align without engaging the canine. Then, after progressing to a relatively stiff arch wire, use a tandem arch wire or spring to engage the canines. This, combined with a stiff base arch wire, will align the canines while not allowing the moment of couple due to the wire angle of entry to influence the rest of the teeth. As the canine uprights, the side effects will not be expressed because the stiff base arch does not allow the deleterious movements.

When an orthodontic practitioner understands wire-bracket relationships and the tooth movements that are a result of these relationships, he or she is better able to predict, and account for, tooth movements that are most likely to occur. This leads to less surprises day to day orthodontic treatment. Lack of surprises makes delivering of orthodontic treatment more enjoyable and rewarding.
1. Mulligan, Thomas. Common Sense Mechanics in Everyday Orthodontics. CSM publishing, 1998. p21
2.Ibid., p24-26
3.Bishara, Samir. Textbook of Orthodontics. WB Saunders, 2001. p333
4. Samson, Gerald. Locomotion 1. www.gnathosce.com
5. Ibid.

Introduction To Muscle Strength
By Dr. Jim Prittinen
When treating orthodontic patients, it is critical to always remember the most important principle of orthodontic treatment. That is, the same brackets, bands, and wires may and probably will produce different treatment responses in different patients. Most of these differing responses occur in the vertical dimension. Throughout this book, I will continually emphasize the importance of vertical control in orthodontic treatment. In fact, controlling the vertical dimension is the most important aspect of orthodontic treatment.
This leads us to the next most important principle of orthodontic treatment, which is the worst mistake that can be made when treating an orthodontic patient is to allow the bite to open in a patient who already has open bite tendencies. The reason this is so important is that no matter the severity of the open bite (and whether it is dental or skeletal), it is typically corrected (unless orthognathic surgery is done) with purely dental movement. Indiscriminate bite opening can lead to aesthetic problems such as excess gingival display, excessive down and back mandibular rotation (which, because the mandible opens on an arc, can result in a retrognathic, class II appearance), and, as a result, poor facial aesthetics. Dr. Sassouni's studies (more on that later) pointed out that the poorest aesthetic results occur in patients with long faces. Since this can be a very poor outcome, we obviously want to avoid this. One of the best ways to avoid it is not to treat open bite patients. Bjork stated in his studies (again, more on that later) that approximately 15% of patients have weak muscled, open bite tendencies. So this is a big part of the 25% of cases that the typical general dentist should avoid.
Diagnosis Of Patients With Open Bite Tendencies
As you will see, there are two general categories of mandibular growth direction.

The first category of growth direction occurs in a patient whose mandible rotates upward and forward with growth (the right photo in the above slide). Other terms that are used interchangeably to describe this growth direction are horizontal growth pattern, counterclockwise growth pattern, or (for reasons that will become apparent later) strong muscled patients. The second category of growth direction occurs in a patient whose mandible rotates downward and backward with growth (the left photo in the slide above). Other terms that are used interchangeably to describe this growth direction are vertical growth pattern, clockwise growth pattern, or (for reasons that will become apparent later) weak muscled patients. Every decision that is made during orthodontic treatment will be influenced by this growth pattern and the patient's muscle strength.
Here is another important concept: very few patients are purely forward or purely backward rotators. In fact, most people exhibit some forward and some backward rotating characteristics. But the most difficult cases to treat are patients who exhibit extreme forward and especially extreme backward growth rotation. If these extreme growth patterns can be identified before beginning treatment, the clinician can assess the difficulty of a particular case. It is vitally important to be able to recognize these extreme growth patterns before beginning treatment.
Diagnosis Of Extreme Growth Patterns
Many orthodontic researchers have done studies which have contributed to the body of knowledge that can be used to diagnose a patient's growth pattern. Let's start by discussing Dr. Sassouni's contribution. Before Dr. Sassouni published his landmark growth studies in the mid 1960’s, good orthodontics was defined as the ability to produce "pretty plaster models".

In other words, occlusion was deemed far more important than facial balance. Dr. Sassouni challenged this traditional view by emphasizing the importance of facial balance. He studied cephalometric x-rays and superimposed soft tissue outlines on these x-rays. By doing this, he was able to identify soft tissue characteristics which reflected skeletal variations. This caused Dr. Sassouni to question of aesthetic values of different facial types. To help discover which facial types were considered aesthetically acceptable and which were considered aesthetically unacceptable, Sassouni constructed a series of shadow profiles; examples of which are shown below.

Sassouni showed these profiles to thousands of people-including lay people as well as dental professionals. He asked these people to comment on the aesthetics of these profiles. The most consistent result in this study was that people disliked the open bite profiles. No matter what other profile characteristics a particular patient had, long faced (open bite) profiles were consistently deemed the most aesthetically unappealing profile by a great majority of the lay and dental professional evaluators.
Keep this study in mind but let's now move ahead about 25 years to a study done by Dr. James McNamara, who is on the orthodontic faculty at the University of Michigan. McNamara has always been interested in the mechanics of Class II correction. But, to effectively and efficiently correct Class II problems, it is important to understand the components of a typical class II malocclusion. In 1990, he did a study in which he tried to identify the components of Class II occlusions. The results of the study showed that almost 90% of class II patients (this was measured by using the mandibular plane angle as well as lower anterior face height) had either ideal or long lower anterior face height. He concluded that vertical control was an important aspect of Class II correction.
By combining these studies, we now know that the most unattractive facial profiles are long face profiles. We also know that most class II malocclusions have vertical dimensions that are either ideal or vertically excessive. Therefore, control in the vertical dimension is vitally important in orthodontic treatment.
The Importance Of Vertical Control
This brings us to what I believe is the most important study ever done regarding orthodontic diagnosis and treatment. It was done by Prof. Arnie Bjork. After practicing orthodontics for 25 years, Prof. Bjork accepted the post of Chairman of the orthodontic department at a Danish University. Once he accepted this position, he never again treated another case but instead focused on this study. This study has become one of the landmark studies regarding facial growth and development.
In this study, Prof. Bjork monitored the growth of 248 children. No treatment was performed on these patients. He took records on these kids every year, but what makes this study so valuable is that he also placed metallic implants in the maxillas and mandibles of these growing children. These implants provided a reliable method of superimposition of the cephalometric x-rays. The main reason that this study is so valuable is that it can never be duplicated because of ethical concerns. Prof. Bjork observed some pretty severe malocclusions as they worsened. In today's environment not treating these cases is unethical because of the harm done to the patient by not treating. Additionally, placing implants in children for observation only would today be unethical, whereas it was not considered unethical in the 1950s when Prof. Bjork performed the study. Note: it is interesting to observe the “crude” technique of implant placement. How will today’s “modern” techniques be viewed 50 years from now?

What did Prof. Bjork conclude from this study? First he postulated that the condyle is the driving force behind craniofacial development and that condylar growth direction depends upon the position of the growth cells which are located on the head of the condyle. This, he felt, is an inherited trait so the amount of mandibular growth is genetically determined. But, how this growth is expressed can be influenced by the control of the vertical dimension of occlusion.
Prof. Bjork stated that if the growth cells are located on the anterior surface of the head of the condyle the mandible will rotate in a forward or counterclockwise direction as growth occurs. Conversely if the growth cells are located on the posterior surface of the head of the condyle, the mandible will rotate in a downward or clockwise direction.


Because of muscle size and the angle at which the muscles work differ in these two growth patterns, the forces of mastication are very different based upon growth rotation. In fact, the forces of occlusion can be up to six times more powerful in forward rotating patients than in backward rotating patients. Because of this, forward rotating patients can be characterized as strong muscled patients and backward rotating patients can be characterized as weak muscled patients. The picture below describes how the muscles work based on angles; it also shows that forward rotating patients have muscles that are stronger because they work in a more efficient direction.

Prof. Bjork also postulated that the location of growth cells can be anywhere on the condylar head, so most patients have some forward and some backward rotation characteristics. For our purposes, it is important to understand that the most difficult orthodontic cases are those patients that show extreme forward rotation (these would be very deep bite patients) and especially extreme down and back rotation (these would be open bite patients). Because the muscles of mastication exert pressure and tension in different areas of the mandible depending on condylar growth direction, the shape or morphology of the mandible differs based upon growth direction. In other words, resorption and apposition of bone and therefore morphology of the mandible differs based upon growth direction. This provides the basis for what Bjork called the structural basis of determining mandibular growth direction. Therefore, growth direction can be predicted based upon mandibular morphology; this can be a very valuable diagnostic tool.

As general dentist practicing orthodontics, it is good to know which cases are going to be the most difficult, so we know what cases are candidates for referral. The structural method of determining growth direction enables us to pick out the most difficult cases because the most extreme forward and downward rotators have more distinctive mandibular morphological characteristics than do patients with more average growth rotation. So, this method identifies the extremes in growth rotation; this can be the basis for deciding whether the case should be referred.
One of the most important aspects of orthodontic diagnosis is to recognize specific structural features that develop as a result of remodeling depending upon the direction of mandibular growth rotation. The rotation pattern can affect treatment. Most orthodontic mechanics are extrusive. Patients with a forward rotating growth pattern (these patients can be referred to as strong muscled patients) have masticatory muscles that can easily resist the extrusive component of most orthodontic mechanics. On the other hand, patients with a down and back rotational growth pattern (these patients can be referred to as a weak muscled patients) are often susceptible to the extrusive component of orthodontic mechanics, because their muscles of mastication cannot overpower the extrusive component of the orthodontic mechanics. Since these weak muscled patients usually already have long faces, this extrusion can be very harmful from an aesthetic and functional standpoint. Remember, Sassouni’s studies show that long faces are undesirable from an aesthetic standpoint.
Extreme forward and extreme backward rotating patients are the most difficult cases to treat. Extreme forward rotators have very strong musculature combined with deep bites; it becomes extremely difficult to overpower the muscle strength to open those bites. Extreme down and back rotators present a different set of challenges. They already have open bite tendencies and because of the weak musculature it is very easy to induce additional bite opening. The structural method of diagnosis allows us to predict the difficulty of managing the vertical dimension based upon the shape of the mandible as viewed on the cephalometric x-ray. This is very valuable diagnostic information.
Always remember the most important principle of orthodontic mechanics. That is, the same brackets, bands and wires will produce different treatment responses in different patients. These different treatment responses are expressed as vertical dimension changes. The patient's muscle strength determines treatment response. Finally, the worst mistake that can be made in orthodontic treatment is to cause bite opening the patient who already exhibits open bite characteristics. By not treating open bite cases, you can never make this mistake. If you decide to treat open bite patients, specific mechanics must be done to help limit the vertical dimension increases.
So what are the morphological characteristics that can be viewed on cephs to help determine the patient's muscle strength? The photograph below shows differing mandibular morphologies.


Here are some of the specific morphological changes that can be used to help make a diagnosis of strong or weak musculature.
The first morphologic characteristic that differs in strong and weak muscled patients is the gonial angle. Strong muscled patients have an acute gonial angle, while weak muscled patients have a gonial angle that is more obtuse. Look at the following slide and note the difference in the gonial angle.

Another characteristic that differs in strong and weak muscled patients is the shape of the lower border of the mandible. Strong muscled patients exhibit a double curvature that resembles a reverse S, whereas weak muscled patients present with a concave lower border.

Symphyseal inclination is another characteristic that can be used to differentiate between strong and weak muscled patients. Strong muscled patients tend to have larger chin buttons than do their weak muscled counterparts. This results in a symphyseal inclination that is acute in strong muscled patients, but more obtuse in weak muscled patients.

Symphyseal radio-opacity or radio-lucency is another distinguishing characteristic. Strong muscled patients tend to have thicker bone, and therefore a more radiopaque appearance, in the symphyseal area. Weak muscled patients are exactly the opposite-their symphyseal area tends to be more radiolucent.

Finally, although it may be difficult to see on a cephalometric x-ray, the inclination of the condyle differs in strong and weak muscled patients. Because the growth cells are located more in the anterior surface of the head of the condyle in strong muscled patients, condylar inclination will be more in an anterior direction. Conversely, because the growth cells are located predominantly on the posterior surface of the head of the condyle on weak muscled patients, condylar inclination will be in a more posterior direction. With the advent of 3D imaging, this characteristic is more observable compared to when viewed on a two dimensional x-ray.

By looking for these characteristics, muscle strength and therefore direction of growth rotation can be predicted. This knowledge (as you'll see later) is vitally important in orthodontic diagnosis.
In summary, patients who exhibit extreme forward or extreme backward rotation have very distinct and different mandibular morphologies. Using mandibular morphology is an excellent diagnostic tool which enables the clinician to pick out the extreme forward and backward rotators. Patients will exhibit extremes in mandibular rotation are the most difficult cases to treat. In extreme forward rotators, the resulting deep bites are often difficult to correct because it is very difficult to overpower the strong muscles of mastication. In extreme backroom rotators exactly the opposite occurs. Open bites are very easily induced. Therefore the same orthodontic mechanics used in strong and weak muscled patients will produce vastly different results in the vertical dimension. This is the most important example of the number one rule in orthodontics-that is the same brackets, bands, and wires may and probably will produce different treatment responses in different patients.
An Orthodontic History Lesson
To further understand some of the basics of orthodontic diagnosis, it is important to understand some of the history of orthodontics. Edward Angle is considered the father of modern orthodontics. He practiced around the turn-of-the-century and was an avowed non-extractionist. His rationale for treating all cases non-extraction was "God made the teeth, God made the bones, therefore they fit". Many of Angle’s students, particularly Dr. Charles Tweed, challenged Angle's insistence on non-extraction in all cases. This shows that the extraction/non-extraction debate is not new. Tweed felt that the best way to ensure long-term stability and facial balance in orthodontic cases was to position the mandibular incisors in an upright position. This required extractions in most cases. Because of Tweed's influence, for most of the 20th century, extraction orthodontics dominated the scene. However, many studies have shown that the long-term stability of both extraction and non-extraction cases are approximately the same. In other words, relapse is just as likely to occur in extraction and non-extraction cases. Furthermore, society's views on what constitutes a balanced face and pleasing profile has changed dramatically over the years. The slide below illustrates how "ideal" facial balance has changed.

Because the concept of the ideal face has changed, non-extraction orthodontics (in other words, positioning the anterior teeth more anteriorly so a full profile is the result) is now much more accepted than it was in the middle and late 20th century.
Despite the fact that the Tweed orthodontic philosophy is not as accepted as it once was, many of the studies carried out by Tweed (and, after his death, his foundation) provide valuable insight into orthodontic diagnosis. One particular study by the Tweed foundation compared successful and unsuccessful class II treatment. This study retrospectively looked at both successful and unsuccessful class II correction cases. The differences in treatment response in successful and unsuccessful cases is significant. In successful cases, results consistently showed forward mandibular rotation and lack of molar eruption.

Conversely, unsuccessful cases exhibited down and back mandibular rotation and significant molar eruption.

In summary, successful cases exhibited minimal backward mandibular rotation while unsuccessful cases exhibited extreme backward mandibular rotation. Although this study showed response to treatment, the mandibular rotation that occurred is very similar to the mandibular growth direction as described by Bjork. Successful cases look a lot like Bjork's strong muscled (forward rotating) patients while unsuccessful cases look a lot like Bjork’s weak muscled (backward rotating) patients. This means that growth can beneficial when the patient is strong muscled and can be deleterious when the patient is weak muscled. This is another reason to be very careful when treating weak muscled patients.
Again, here are the concepts that Bjork's studies emphasized. The mandible, although strictly speaking is not a long bone like leg or arm bones, grows like one. The amount of growth is genetically determined. How this growth is expressed can be influenced by the control (or lack of control) of the vertical dimension of occlusion. Therefore, to avoid the unsuccessful results as demonstrated in the Tweed Foundation study, one of the major goals of orthodontic treatment is control of excessive molar eruption. This will help minimize backward mandibular rotation. Here's another way of looking at it: the mandible is a beast; it's going to grow no matter what. Our job is to control the direction of growth; the best way to do that is by controlling the vertical dimension of occlusion. Controlling this vertical dimension is much easier in strong muscled patients than in weak muscled patients. To make things easier on yourself, simply refer weak muscled patients. If you feel you are up to the challenge of treating weak muscled patients, use mechanics to help limit excess molar eruption.
Intra Matrix Rotation

In his studies, Bjork also discussed the concept of intra matrix rotation. He defined the intra matrix as the maxillary and mandibular teeth and alveolar processes. The intra matrix rotates in conjunction with, but independent of, the maxilla and mandible. To understand intra matrix rotation, one more definition is necessary. That is the fulcrum. Bjork described the fulcrum as the most anterior portion of the dentition where contact between the maxillary and mandibular teeth occur.
There are three basic types of intra matrix rotation. Type I occurs in strong muscled patients when the fulcrum is at the incisal edges of the upper and lower anterior teeth. This combination of mandibular and intra matrix rotation results in optimal downward and forward growth rotation. If a patient presents with this set of characteristics, the only possible malocclusion possible is a class I crowded situation. The slide below shows an example of a type I intra matrix rotation.

Type II intra-matrix rotation occurs in strong muscled patients where the fulcrum has shifted to the middle of the arch. Because there is nothing preventing anterior eruption, a dental deep bite as a result of excess anterior eruption is often the result of type II intra-matrix rotation. Patients who experience this type of intra-matrix rotation present with class II division II characteristics of occlusion. An example of this is presented in the slide below.

An important question when dealing with this type of intra-matrix rotation is "why does the fulcrum shift?" There are many reasons for a fulcrum shift. They include allergies, airway or breathing problems, tongue, lip and/or finger habits and early loss of primary teeth. These problems (which are mostly environmental) can greatly influence the expression of mandibular growth.
This brings us to the last general category of intra-matrix rotation, which can be called a type III intra matrix. This occurs in weak muscled patients when the fulcrum is in the posterior segment of the arches. The reason for this fulcrum shift could be genetic (down and back mandibular rotation would naturally produce the posterior fulcrum) or environmental (the same reasons as described for a type II intra matrix). No matter what the reason for the shift, this growth pattern can result in two possible outcomes. If the rotation pattern is combined with optimal anterior eruption the result will be a long face but reasonably good occlusion. However, if this rotational pattern is combined with less than optimal anterior eruption, the result will be a skeletal and dental open bite, as seen in the slide below.

With all of these variations in growth and intra matrix rotation patterns, it becomes easy to see why treatment response in different patients (remember the number one rule) occurs. The slide below shows two different patients, one of whom experienced extreme forward mandibular growth rotation with the fulcrum not at the incisal edges of the anterior teeth, and the other who experienced down and back mandibular growth rotation with less than optimal anterior eruption. Everything about these cases is different; do you really expect treatment response to be the same?

Before we end this basic science discussion, one more concept needs to be emphasized. This concept is that all faces flatten as they mature, but the mechanics of flattening differ in forward and backward rotators. It is important to understand that significant flattening of the face occurs as kids grow. When completing a phase 1 treatment, if the patient looks very full, the natural changes to the face that occur as a result of normal development will lead to better facial balance. So, if given the choice, finish phase 1 treatments with the patient looking a little full because that fullness will resolve itself as growth is expressed.
In strong muscled patients, because of the direction of mandibular growth rotation, the chin moves forward but the strong facial musculature prevents the teeth and alveolar processes from moving forward as much as the chin. The result is a flatter face as the patient matures. Look at the slide below to see an example of this phenomenon.

This patient was treated non-extraction; notice the facial changes which naturally occurred as she matured.
In weak muscled patients, faces also flatten but the mechanics are different than those that occur in strong muscled counterparts. Mandibular rotation causes down and back movement of the chin and the retrusive position of pogonion results in a flatter face. The patient shown in the slide below demonstrates this phenomenon.

In conclusion, to effectively treat orthodontic patients, the clinician must understand growth rotation of the mandible and how it affects orthodontic treatment. By studying the work of Sassouni, McNamara, Bjork as well as many other orthodontic researchers, the orthodontic clinician can achieve a good working knowledge of mandibular growth rotation and how this relates to growth and development.

Dr. Prittinen received his DDS degree from the University of Minnesota in 1981. He has been an orthodontic instructor for the United States Dental Institute since 1993 and is a member of the American Orthodontic Society (AOS). In addition, he has been the director of Practical Orthodontics since 1997. Practical Orthodontics is an organization whose mission is to provide orthodontic education opportunities for dentists. Dr. Prittinen maintains a general dental practice in Virginia, MN, where he treats about 50 orthodontic cases per year. Dr. Prittinen has had numerous orthodontic articles and reviews published in “General Dentistry”, the AOS Journal, and many other publications. His website, www.practicalorthoce.com, is a site dedicated to providing orthodontic education to general practitioners who want to learn more about orthodontics.